Abdominal Distension and Treatment of Colon (Enema – Purpose, Classification, Methods, Procedure and After Care of Patients)
It is accumulation of excessive amounts of flatus, liquid or solid intestinal contents.
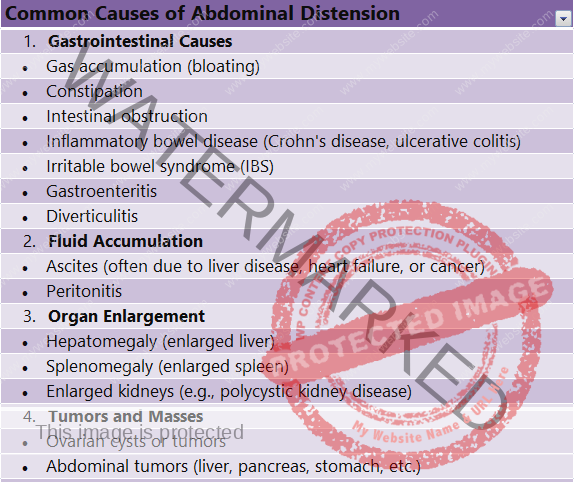
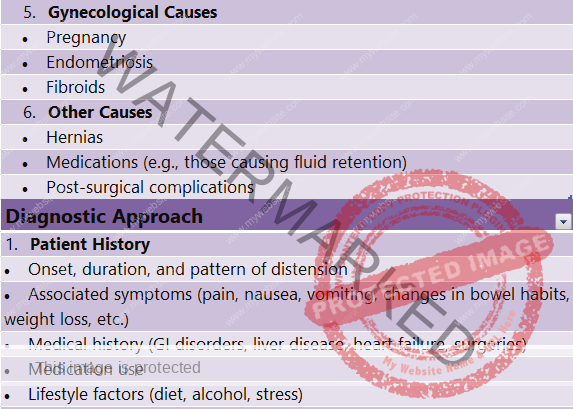
Causes of Abdominal Distension
An obstruction that blocks the passage of flatus and intestinal chime or faeces. Obstruction can occur due to paralytic ileus or abdominal tumors.
Long periods of bed rest or relative inactivity can slow peristalsis and cause distension.
Surgery involving bowel manipulation, especially bowel surgery can cause decreased peristalsis leading to distension.
Constipation and faecal impaction also can cause distension.
TREATMENT OF COLON
To soften hard faecal matter e.g., oil enema.
Enema
An enema (plural – enemas, enemata) is an introduction of fluid into the lower bowel through the rectum for the purpose of cleansing or to introduce medication or nourishment
Purpose of Enema
To stimulate defecation and to treat constipation e.g. simple evacuant enema.
To administer medications e.g., sedative enema.
To protect and soothe the mucus membrane of the intestine and to check diarrhea e.g., emollient enema.
To destroy intestinal parasites e.g., anthelmintic enema.
To relieve gaseous distension e.g., carminative enema.
To administer fluids and nutrients e.g., nutritive enema.
To relieve inflammation e.g., astringent enema.
To induce peristalsis e.g., purgative enema.
To stimulate a person in shock and collapse e.g., stimulant enema.
To reduce temperature e.g., cold enema or ice enema.
To clean the bowels prior to X-ray studies, visualization of the bowel, surgery on the bowel or delivery of a baby e.g., saline enema.
To make diagnosis e.g., barium enema.
To establish regular bowel functions during a bowel training programme.To induce anesthesia e.g., anaesthetic enema.
Classification of Enema
It is classified into two:
1. Evacuant Enema
2. Retained Enema
Evacuant Enema is classified into
1. Simple evacuant enema
2. Cold enema
3. Medicated evacuant enema.
Medicated evacuant enema is classified into
1. Oil enema
2. Purgative enema
3. Astringent enema
4. Anthelmintic enema
5. Carminative enema.
General Instructions for Giving Enema
1. The appropriate size catheter or rectal tube need to be used. For giving a cleansing enema use no. 22 French for adults, no. 12 French for an infant and no.14 to 18 French for the school age child.
2. The rectal tube needs to be smooth and flexible. Any tube with a sharp or ragged edge should not be used because of the possibility of damaging the mucus membrane of the rectum.
3. The rectum tube is lubricated with a water soluble lubricant or with Vaseline to facilitate insertion and to decrease irritation of the rectal mucosa. Use only a small amount to prevent blockage of the tube.
4. The temperature of the solutions needs to be adjusted according to the purpose of the enema. To give an evacuant enema, the temperature should be between 40.5 to 43 degree celcius for adults and 37.7 degree celcius for children. A retained enema should be given at the body temperature.
5. The amount of the solution to be administered depends upon the type of the enema and the age and size of the person. For giving evacuant enema use 500 to 1000 ml for adults, 250 to 500 ml for a child and 250 ml or less for an infant.
For giving retained enema, the quantity given at a time should not be more than 100 ml to 150 ml so that the rectum will not be distended to cause peristaltic movement.
6. When an enema is administered, the client usually assumes a left lateral position. In this position, the position of the sigmoid colon is below the rectum, thus facilitating instillation of the fluid. For a high cleansing enema, the client changes position during the administration of the enema from left lateral to dorsal recumbent and then to right lateral. In this way the entire colon will be reached by fluid. For an evacuant enema the bed should be made flat and for a retained enema the foot end should be raised.
7. The distance to which the tube is inserted depends upon the age and the size of the client. For an adult it is normally inserted 7.5 to 10 cm (3 to 4 inches). If any obstruction is encountered, it should be withdrawn and reported.
8. The height of the can should be adjusted to regulate the flow of the solution according to the type of the enema administered. For cleansing enemas, the height of the can should not be above 18 inches ( 45 cm) from the anus and for retention enemas, it should not be above 8 inches (20 cm) from the anus. The higher the container, the greater is the force with which the solution flows into the rectum. There is an increase of 0.5 lb of pressure for every 12 inches of elevation.
9. The length of time that the enema solution is retained will depend upon the purpose of enema and the ability of the client to contract the external sphincter to retain the solution. Oil retention enemas are usually retained for 2 to 3 hours. Other cleansing enemas are normally retained 5 to 10 minutes. To assist a baby to retain the solution, the nurse can press the baby’s buttocks together, thus providing pressure over the anal area.
11. Make sure the whole apparatus used for the administration of enemas is in a good working condition.
12. Regulate the flow of fluid according to the type of the enema: give retention enemas very slowly, usually by a Murphy drip. Before giving cleansing enemas, regulate the flow of fluid and pinch the tube before the tube is inserted into the rectum.
13. If the rectum is impacted, attempt to remove the faecal matter with a gloved finger. The bowels should be cleaned out by a simple enema before giving retention enema.
Prevent air from entering into the rectum:
By removing the froth from the solution
By expelling air from the tube
By not letting the fluid run in completely from tube
14. Listen to the complaints of the client and should not ignore any discomfort however small they are.
15. Prepacked enemas will have their own instruction which need to be followed unless there are other instructions from the physician.
Simple Evacuant Enema (Large Enema to be Expelled)
Purpose:
To stimulate defecation and to treat constipation
To relieve gaseous distension by stimulating the peristalsis
To relieve retention of urine by reflex stimulation of the bladder
To stimulate uterine contractions and to hasten the child birth
To cleanse the bowel prior to X-ray studies, visualization of the bowels (e.g., sigmoidoscopy), surgery and retention enemas
Solutions Used
Soap and water: soap jelly 50 ml to 1 litre of water.
Normal saline: sodium chloride 1 teaspoon to half litre of water
Tap water
Amount of Solutions to be used
Adults – 500 to 1000 ml (1 to 2 pint)
Children – 250 to 500 ml (0.5 to 1 pint)
Infants – 250 ml or less
Temperature of the Solution
Adults – 40.5 to 43 degree celcius
Children – 37.7 degree celcius
Oil Enema
These are given to soften faecal matter in case of severe constipation, before the first bowel movement after operations on the rectum and perineum, to avoid straining and injury to the sutures and wounds. It should be retained for half an hour to 1 hour to soften the faeces. It should then be followed by a soap and water enema to open the bowels.
Solutions Used
Olive oil
Gingerly oil or sweet oil
Castor oil and olive oil (1:2)
Amount of solutions to be used: 115 to 175 ml
Temperature of the solutions: 37.7 degree celcius
Purgative Enema
These are given to cause the bowel to contract actively and to evacuate its contents. It acts by their irritating effect on the mucus lining, stimulate peristalsis and cause evacuation of the bowel. It also acts as a hygroscopic substance – it draws water itself. The stretching of the intestine due to this inflow of fluid causes the intestine to contract and leads to the evacuation of the bowel.
Solution Used
Pure glycerin – 15 to 30 ml
Glycerin and water – 1:2
Ox gall – 15 to 30 ml
Glycerin and castor oil – 1:1
Magnesium sulphate : 60 to 120 ml with sufficient amount of water to dissolve it
1-2-3 enema: magnesium sulphate 30 ml, Glycerin 60 ml, and water 90 ml
Amount and temperature of the solution is that of oil enema.
Carminative Enema (Antispasmodic)
These are given to relieve gaseous distension of the abdomen by causing peristalsis and expulsion of flatus and faeces. It is given as simple evacuant enema.
Solutions Used
Turpentine: 8 to 16 ml of turpentine mixed thoroughly with 600 to 1200 ml of soap solution.
Tr. Asafoetida: 8 to 18 ml of Tr. Asafetida mixed thoroughly with 600 to 1200 ml of soap solution.
Milk and molasses: 90 to 230 ml of molasses well mixed with equal quantity of warm milk.
Anthelmintic Enema
This is given to destroy and expel the worms from the intestines. Before the treatment is given, the bowel should be cleansed by a soap water enema so that the drug may come in direct contact with the worms and the lining of the intestines. The treatment is given until the worms are destroyed.
Solutions Used
Infusion of quassia: 15 gms of chips to 600 ml of water.
Hypertonic saline solutions: sodium chloride 60 ml with 600 ml of water.
Amount of the solution: 250 ml.
Astringent Enema
It contracts the tissues and blood vessels, checks bleeding and inflammation, lessens the amount of mucus discharge and gives a temporary relief in the inflamed area. It is usually given in colitis and dysentery. They are usually given in the form of rectal or colonic irrigations. The solution is allowed to run in slowly and return quickly to avoid distension, pain and irritation of the inflamed well.
Solutions Used
Alum: 2 gms to 600 ml of water
Silver nitrate 2 %: silver nitrate dissolved in the distilled water.
Temperature of the solution: it is given as hot as the client can stand.
Cold Enema (Ice Enema)
This is given to decrease the body temperature in hyperpyrexia and heat stroke. It is given in the form of colonic irrigation.
Complications
Hypothermia
Abdominal cramps
Retention Enema
2. Check the date and type of surgery
Stimulant Enema
A stimulant enema is given in the treatment of shock and collapse. It is also sometimes given in case of poisoning, e.g., coffee enema is given in cases of opium poisoning.
Solutions Used
Black coffee: one tablespoon coffee powder to 300 ml of water
Brandy: 15 ml of brandy added to 120 to 180 ml of glucose saline.
Amount of solution: 180 to 240 ml.
Temperature of solution: 42 to 43 degree celcius
Sedative Enema
It is a retention enema containing a sedative drug given to induce sleep.
Drugs Used
Paraldehyde
Chloral hydrate
Potassium bromide
Dose: as ordered by the doctor.
Anaesthetic Enema
It is a retention enema containing an anaesthetic drug to produce anaesthesia in the client.
Drugs Used: Avertin 150 to 300 mg per kg of body weight.
Emollient Enema
This is the introduction of bland solution into the rectum for the purpose of checking diarrhea or soothing and relieving irritation on an inflamed mucus membrane.
Solutions Used
Starch and opium: Tr. Opium 1 to 2 ml added to 120 to 180 ml of starch mucilage or rice water.
Starch mucilage alone
Amount of solution: 120 to 180 ml
Temperature of solution: 37.8 to 40.5 degree celcius
Nutrient Enema
It is a retention enema to supply food and fluids to the body. Selection of the fluids depends upon the ability of the colon to absorb it. Nutrient enema is particularly useful in conditions like haemophilia which makes I.V. infusion difficult or undesirable.
Solutions Used
Normal saline
Glucose saline – 2 to 5%
Peptonized milk – 120 ml
Amount of solution – 1100 to 1700 ml in 24 hours or 180 to 270 ml at 4 hourly intervals
Temperature of solution – 37.8 degree celcius
Methods Used in Giving Enemas
Using enema can and tube
When large amounts of fluids are to be given, this method is used e.g., soap and water enema.
Funnel and catheter method
When a small quantity of fluids are to be given, this method is used e.g., oil enema.
Glycerin syringe and catheter method
When a small quantity of fluid is to be given, this method is used e.g., purgative enema.
Drip Method
When the fluid is to be administered very slowly in order to aid in its absorption e.g., nutrient enema
Giving Enema, using Enema-Can and Tubing
Preliminary Assessment
1. Check the diagnosis
3. Check the abilities and limitations concerning movements
4. Check the consciousness and the ability to follow direction
5. Check the nature of enema ordered and special precautions, if any, to be followed.
6. Check the general condition of the client and the ability to retain the fluid.
7. Check the medical order for the collection of stool specimens if any, for laboratory tests.
8. Check for any lesions on the rectal and perineal area.
9. Any extra help needed e.g., to place the bedpan in position
10. Articles available in the client’s unit.
Articles
A tray containing
1. Enema can, tubing, glass connection, screw clamp etc
Purpose: to prepare the solution and adjust the rate of flow
2. Rectal tube (adults) or rectal catheter placed in a kidney tray
Purpose: to introduce into the rectum
3. Mackintosh and towel
Purpose: to protect the bed
4. Water soluble jelly or Vaseline
Purpose: to lubricate the tube
5. Rag pieces in a container
Purpose: to apply the lubricant and to clean the perineum when necessary
6. Hot and cold water in jugs
Purpose: to prepare the solution
7. Soap jelly in a bottle
Purpose: to prepare the solution
8. Ounce glass
Purpose: to measure the soap jelly
9. Paper bag
Purpose: to discard the wastes
10. Specimen bottles (if needed)
11. Bedpan (2) or commode
Purpose: the first one to receive the contents of the bowel and the second one to give the perineal care
12. Clean linen as needed
Purpose: to change the linen after the procedure
13. Toilet tray
Purpose: to clean the perineum
14. I.V. stand or overbed table
Purpose: to hold the enema can in position
Preparation of the Client and the Unit
1. Explain the procedure to the client to win his confidence and cooperation. Explain the discomfort caused by the enema fluid and the need for retaining the solution for some time.
2. Provide privacy with curtains
3. Cover the client with a sheet or bath blanket and fanfold the top linen to the foot end of the bed
4. Remove the back rest and pillows.
5. Place the mackintosh and towel under the client’s buttocks to protect the bed and the linen.
6. Place the client in a left lateral position with the buttocks close to the edge of the bed.
7. Keep all articles arranged on the bedside locker
8. Keep the bedpan under the bed over a paper or stool
9. Adjust the I.V. pole or overbed table to hold the enema can at the required height.
10. Remove bottom garments or raise it above the waist level.
11. Drape the client immediately before giving the enema. Fold back a small portion of the sheet or the bath blanket, covering the client to expose only the anus.
Procedure
Steps of Procedure
1. Wash hands
Reason: to prevent cross infection
2. Attach the tubing to the enema can and clamp the tube
Reason: to prepare the solution and be ready for the administration
3. Prepare the solution at the required temperature. Add 30 ml of soap jelly to 600 ml of water. Test the temperature of the solution at the inner aspect of the wrist. Remove the forth from the can.
Reason: temperature above 43 degree celcius may injure tissues and temperature below 21 degree celcius may produce severe cramping.
4. Hang the can with the solution on the stand and adjust the height at 45 cm from the anus.
Reason: the rate of flow and the pressure of the fluid will increase according to the height of the can.
5. Attach a rectal tube to the tubing. Loosen the screw clamp and let a small amount of fluid to run into the kidney tray. Regulate the flow of the solution by adjusting the screw clamp. Pinch the tubing with fingers. Read the level of the fluid in the enema can.
Reason: running the fluid through tube will help to expel the air from the tubing and make sure that the whole apparatus is in working order. Reading the level of the fluid can help us to calculate the amount of fluid introduced into the rectum.
6. Lubricate the tip of the rectal tube about 2 to 4 inches from the tip. Lubricant is applied to the minimum with a rag piece.
Reason: lubrication of the tube will prevent friction. The lubricant should not block the tube.
7. Separate the client’s buttocks to visualize the anus clearly and insert the tip 8 to 10 cm gently while the client exhales a deep breath.
Reason: forceful insertion of the rectal tube may injure the anal or rectal tissue.
8. Hold the enema tube in place while releasing the pressure on the tube and let the fluid run in. Read the level of the fluid and make sure that is flowing.
Reason: holding the tube throughout the procedure will prevent the displacement of the tube.
9. During the administration of the fluid ask the client to take panting breaths.
Reason: breathing will open mouth relaxes the abdominal muscles, decreases pressure on the colon. Also distract the client enough to relax abdominal muscles.
10. Temporarily stop the administration of the solution (should not remove the tube before the desired amount of solution has gone in) if the client has an urge to defecate or has abdominal cramps or if the solution level is rising in the enema can.
Reason: temporary stoppage of the fluid will relax the bowels as the peristaltic movement is passed off.
11. Continue the fluid administration to give about 500 to 1000 ml of solution. Stop the procedure if the client develops discomfort.
Reason: large amount of faeces in the colon decreases the volume of the solution retained comfortably.
12. Clamp the tubing. Gently remove the rectal tube by pulling it through 3 to 4 layers of rag pieces. Hold the rag pieces around the tube and firmly against the anus.
Reason: holding the rag pieces around the tube cleanses the tube by removing the faeces from the tube. The pressure applied on the anus will help the client to maintain the control of the anal sphincter.
13. Discard the rag pieces in the paper bag. Detach the rectal tube and place it in the kidney tray.
Reason: avoid contamination of the articles and environment, with the soiled articles.
After Care of the Patient and Articles
1. Encourage the clients to retain the fluid for 10 to 15 minutes. Encourage slow breathing with open mouth for relaxation.
2. Turn the client on the back and assist him onto toilet, commode or bedpan.
3. Give a call signal to the client and leave him alone for sometime if safe.
4. Observe enema results, noting the color, consistency and the amount. Obtain specimens if desired.
5. Bring the toilet tray and assist him for perineal care. If bedpan is used, the second bedpan is placed under the buttocks before the perineal care
6. Remove the bedpan, dry the client, put on the garments, change the bed linen if needed, straighten the sheets and adjust the position of the client in the bed to make him comfortable.
7. Explain the client that he may need to evacuate the bowels several times in the next few hours.
8. Take the bedpan to the sanitary annex, inspect the contents, empty the bedpan, clean it and keep it on the bedpan rack ready for the next use.
9. Take all articles to the utility room. Disinfect the rectal tube, clean it and boil it and store it in its proper place in the proper manner. Tidy up the client’s unit.
10. Wash hands.
11. Record the type of enema, the result, the untoward results observed, if any, with date and time on the nurse’s record.
12. Return to the bedside. Evaluate the client’s condition and comfort. Take vital signs if the client is pale and sweating. Report immediately and get medical aid for the client.
Send the specimens if any, to the laboratory.
Giving Enema with Funnel and Catheter e.g. Oil Enema
Small enemas to be expelled are given using funnel and catheter. The oil is kept warm by placing the container in a bowl of warm water. During the administration, the height of the funnel should not be more than 8 inches from the anus. Help the client to retain the solution either by raising the foot end or by pressing buttocks. The oil enema is to be retained for 2 to 6 hours to soften the faecal matter. It may be then followed by a soap and water enema to expel the faecal contents. The preparation and after care of the client and articles are same as in soap and water enema.
Giving Enema using a Glycerin Syringe e.g., Glycerin Enema
A glycerin syringe (metal syringe) and a rubber catheter attached to its nozzle are used. Air is to be expelled from the syringe and the tube, prior to the administration of the fluids. This method is particularly useful for giving enema to children.
Giving Enema by the Drip Method e.g., Nutrient Enema
(Proctoclysis or Continuous Retention Enema)
Articles Required
All the articles are used for an evacuant enema (except: reservoir, tubing attached to the reservoir, Murphy drip and a clamp, fine catheter, bed blocks to raise the foot end)
The administration of a retention enema is done by the drip method. The main purpose of the procedure is that the solution is to be retained and should never be evacuated. A fine catheter is used in the place of a rectal tube to diminish the stimulation of the defecation reflex. The reservoir is raised above the anus only far enough to allow the solution to run slowly into the rectum or the flow is regulated by a Murphy drip and a clamp ( to less than 40 drops per minute) because administration of a large amount of fluid at a time will distend the rectum, causing defecation. The foot end is raised to retain the fluid.
Usually a retention enema is preceded by a simple enema to keep the bowels free of faecal matter to aid absorption of fluids and drugs.
SUPPOSITORIES
Suppositories are solid, cone shaped or oval shaped masses that melt at body temperature. There are several varieties of suppositories available e.g., glycerin suppositories, dulcolax suppositories. Some act as a local irritant which stimulates secretion by the mucosa, while others act directly on the nerve endings and stimulate peristalsis. The suppositories are to be kept in the refrigerator, because they melt at room temperature and insertion becomes difficult.
Before introducing suppositories, explain the procedure to the client. The client is placed in a comfortable position, usually left lateral. Suppository is removed from its package and held in the right hand between the two fingers (the nurse wears a glove on a finger cot). Separating the buttocks with the left hand insert the suppository into the anus. Once it has passed the external sphincter, advance it beyond the internal sphincter, pushing it with the index finger, otherwise the suppository will be expelled from the anal canal. The nurse should make sure that the suppository is positioned to the side of the rectum against the mucosa, rather than in the faecal matter, because the intended action of the medication is on the intestinal wall. The client should be instructed to retain the suppository as long as it is comfortable – about 20 to 30 minutes or even longer.
INSERTION OF A FLATUS TUBE
A rectal tube inserted into the rectum relieves the flatulence and gaseous distension of the abdomen. Prepare the client as for an enema. Place the client in a comfortable position. Lubricate the flatus tube and introduce 4 to 6 inches into the anus canal while the free end of the tube being kept under the water in the kidney tray. Watch for the expulsion of the gas which is seen bubbling through the water. The tube is left in place for not more than 20 minutes; longer periods of insertion can lead to permanent sphincter damage. The tube can be re-inserted every 3 to 4 hours, if necessary.
This information is given for educational purpose. This information is provided for educational and informational purposes only and does not constitute providing medical advice or professional services. The information provided should not be used for diagnosing or treating a health problem or disease, and those seeking personal medical advice should consult with a licensed physician. Always seek the advice of your doctor or other qualified health provider regarding a medical condition.